Background
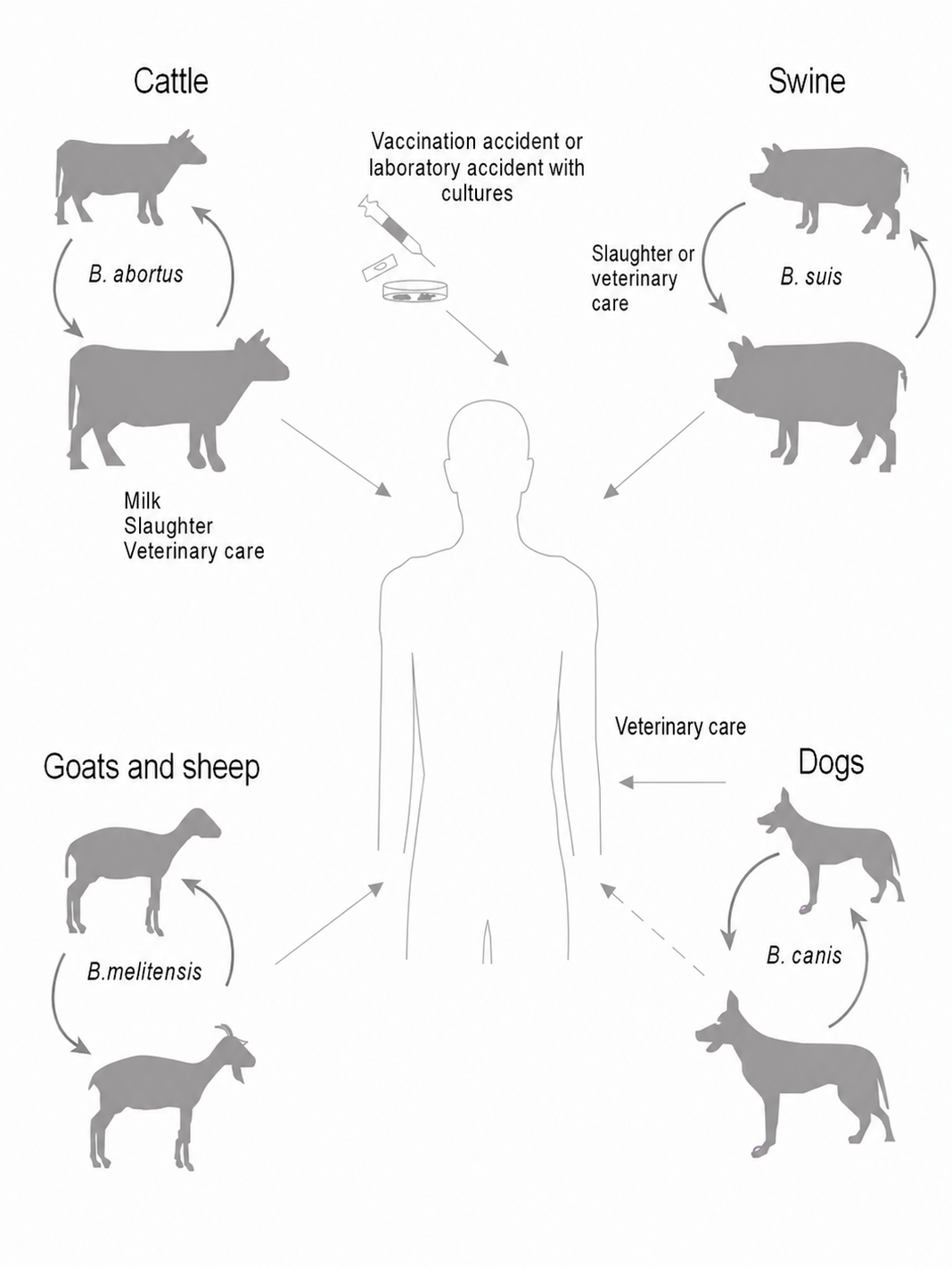
Brucellosis is a worldwide zoonotic disease caused by bacteria of the genus Brucella, affecting both domestic and wild animals as well as humans. The most relevant species include Brucella melitensis, mainly associated with sheep and goats, Brucella abortus, primarily linked to cattle, and Brucella suis, mainly related to swine. Although each species has its main reservoir, infection is not strictly host-specific and may be transmitted to other species under suitable conditions.
In animals, infection is usually chronic and is associated with abortion, infertility, and bacterial shedding through uterine secretions, placenta, colostrum, and milk. In humans, transmission occurs mainly through direct contact with tissues or fluids from infected animals, consumption of raw milk or unpasteurized dairy products, and also in certain occupational settings such as laboratories or slaughterhouses. From a clinical perspective, human brucellosis may have a variable incubation period and present with continuous or intermittent fever, sweating, headache, weakness, chills, weight loss, and other non-specific symptoms, which can make recognition difficult.
The disease remains particularly relevant in the Mediterranean region, Africa, the Middle East, Asia, and Latin America, where it represents an important challenge for both public health and animal health. In this context, serological diagnosis plays an essential role in the initial approach to brucellosis in both humans and animals, and may be complemented by bacteriological methods or other confirmatory techniques depending on the clinical case.
Product features
BRUCELLACAPT®, in an easy and simple way, allows for the detection of antibodies from advanced stages of the illness. This product has been specially designed for the diagnosis of chronic brucellosis.
As showed in scientific literature, a rapid reduction of BRUCELLACAPT® titers, together with an improvement in clinical parameters, is a good indicator of patient recovery.
Perfect serological technique for the brucellosis diagnosis, especially in evolved phases, and also for treatment follow-up.
Fast and simple performance. Visual reading in 24 hours.
It does not require washing nor pre-dilution of the samples.
Highest sensitivity and specificity.
International recognition shown in scientific literature.
Allows for screening and titration protocols.

Diagnostic recommendations
Results should always be interpreted together with clinical evaluation, epidemiological exposure, disease stage, immune status and other diagnostic procedures.
Brucellosis diagnosis should not rely on a single laboratory result. Whenever possible, serology should be interpreted together with culture, molecular methods, follow-up samples and clinical findings.
Early samples may be negative because antibodies may not yet be detectable. If clinical suspicion remains high, a second sample should be obtained 14–21 days later and tested in parallel with the first sample to assess seroconversion.
A negative serological result does not always exclude brucellosis, particularly in early infection, localized disease or immunosuppressed patients.
Rose Bengal detects agglutinating antibodies and may produce false-negative results in localized or prolonged disease when non-agglutinating antibodies predominate.
False-positive Rose Bengal results may occur in people living in endemic areas, in individuals with previous Brucella infection, or in infections caused by bacteria sharing common LPS epitopes with Brucella.
IgM is useful for acute forms of brucellosis, but low IgM levels may occasionally persist for more than 12 months after infection. IgM should not be interpreted alone.
For IgM ELISA testing, human IgG sorbent must be used to avoid possible false-positive results due to rheumatoid factor or false-negative results due to excess IgG antibodies.
BRUCELLACAPT® titres higher than 1/320 suggest brucellosis, but results should always be evaluated according to clinical evidence and local seroprevalence.
In endemic areas, lower BRUCELLACAPT® titres may be encountered and require cautious interpretation.
In positive BRUCELLACAPT® titres of 1/5120, additional serum dilutions should be tested, especially when the assay is used for patient follow-up.
A decrease in BRUCELLACAPT® titres may support patient recovery when accompanied by clinical improvement, but serological follow-up should not be used as the only criterion of cure.
Serological assays do not indicate the site of infection and are not intended to replace culture or direct diagnostic techniques.
PRODUCTS
BRUCELLACAPT®
Analytes: Brucella
SERUM DILUENT FOR BRUCELLACAPT®
MORE RESOURCES

Related germs and organisms categorized for this product line.

Downloadable PDF materials, brochures, and technical documents.


The latest insights, news, and research articles from our scientific team.

Understanding the complexity of vaginal infectionsVaginal infections are among the most frequent reasons for gynecological consultation, but their dia...

Beyond detection: H. pylori testing in today’s laboratory workflow
Helicobacter pylori remains a highly relevant target in gastrointestinal diagnostics. It is a familiar pathogen, but its clinical importance has not d...

Aspergillus galactomannan: a practical biomarker for invasive aspergillosis diagnosis
Invasive aspergillosis is still one of the most difficult fungal infections to diagnose early. It mainly affects patients with weakened immune systems...

Scientific bibliography and references related to this product.